Ankle and Knee Pain when Running Downhill
- Dr Abbie Clinics
- May 28, 2018
A 35 year-old male attended Dr. Abbie Clinics suffering left ankle pain and knee pain in both knees following running activities, reporting it was worse when running downhill.
On assessment using our unique Najjarine Biomechanical Assessment (NBA), we found the following:
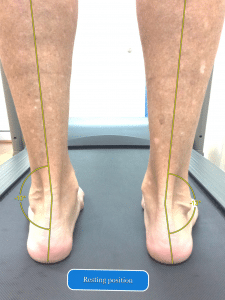
- The patient has what is termed internal tibial torsion (pigeon toed angle), which is a
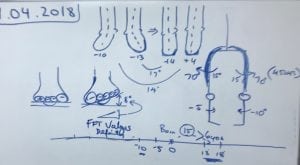


- On assessment the hip movement is 70 deg outward movement to 15 deg inward movement. The ideal measurement should be 45=45 deg each way. This means the gluteals and the whole external hip rotators are tighter than the groin muscles to counteract the pigeon toed position. Hence below the knee, the shin turns in and above the knee, the femur or upper leg bone turns out, causing the knee pain and unnecessary rotational on the knees (see diagram).
- Both feet pron




Treatment
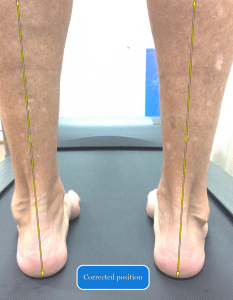
- Cast the feet in the ideal position which is the weight bearing position. Prescribe orthotics devices, one for running and one for every day use (most people wear the same orthotics for activity and general walking). In running the force on the feet is about 4-5 times the body weight and the material and angles in running orthotics are different to those for general walking.
- In the cast, apply a forefoot wedge on the left foot only to accommodate the forefoot valgus to prevent lateral ankle sprains and also assist in downward hill running to prevent abnormal or overuse lateral foot loading.
- Internal tibial torsion ( pigeon toed) cannot be corrected at his age, but it is recommended to treat children whilst they are growing to correct pigeon toed.
- The patient will also need to strengthen his VMOs and stretching his gluteals and ITBs.
- Also recommended that patients need foot mobilised. When it comes to the left foot lateral ankle sprains, most likely the cuboid bone can sublux (partially dislocate) seen on X-ray or can be felt by a trained practitioner. This can cause swelling and pain on the outer ankle and foot position.
- It is also important to treat the outside shin muscles with dry needling or deep tissue massage to break down unnecessary scar tissue. This is because the peroneal muscles (outside shin muscles) had to elongate further to reach the forefoot to the ground.
Extra information
Because of gravitational forces on our body and ground reaction forces opposing. There are important engineering principals that have to be taken into consideration when casting and making custom made orthotic devices.
Dr. Abbie Clinics founder, Dr Abbie Najjarine, could not understand why casts were usually taken in a laying or sitting position and orthotics made for when the patient is in a laying position, even though this system may have served and assisted practitioners for many years. Technology changes – cars made 50 years ago are different to the cars driven today.
Dr Abbie was the pioneer in his field for using standing casting method with engineer principles to perfect his treatment techniques. He found treatment of his patients improve dramatically after perfecting the art of casting. He was also the first in Australia to use computer casting back in 1991 and was the first in Australia to use computer generated orthotics. For the last 30 years he has only taken cast in a weight bearing position with positive results.
Dr Abbie has trained over 20,000 practitioners world wide and still use his method with great results and says that assessment and ccurate casting are of utmost importance. Also knowing the correct orthotic devices to prescribe is key as well as what other treatment modalities might be needed is necessary when treating with orthotics.
People forget we walk on unnatural unyielding surfaces in our society. Over 100 years ago we may have walked on natural surfaces and different terrain, using our muscles effectively. These days everyone walks on hard ground and we are seeing an increase in osteoarthritis and joint replacement in our society.
When you run on hard ground the force is 4-5 times the body weight. Newton’s third law says that in simple terms, for every action there is an equal and opposite reaction.
Orthotics
We also found that the patient has a forefoot valgus deformity (bunion) only on the left foot, which is a congenital condition we cannot change, and they have a 8 degrees forefoot angle.
A Forefoot Valgus is the classic case of causing sprained ankles. So this must be accommodated in the orthotics device prescribed, designed to change the ground to suit us individually – just the same way when glasses are prescribed.
There are different orthotics devices from pre-made, to mild correction, then to full correction, depending on the condition and they range in prices.
Othotics are made with different materials and different densities depending on the patient’s condition.
At Dr. Abbie Clinics we have about 28 styles of orthotics with about 100 different modifications that can be applied to the orthotics depending on the assessment. There are also different casting methods from plaster casting , impression casting and computer casting all depends on the biomechanical assessment of the patient.
